Controlled Comparative Study of Post-operative Analgesic Effect of Pre-emptive use of Pregabalin & Ketorolac in Patients Undergoing Single Level Decompressive Lumbar Laminectomy
Abstract
Background: Pre-emptive analgesia helps to reduce the physiological consequences of nociceptive transmission. Pregabalin has anti-convulsant, anti-hyperalgesic, and anxiolytic properties and Ketorolac is a nonsteroidal anti-inflammatory drug (NSAID) with potent analgesic effects and a relatively low incidence of side effects. The aim is to assess and compare post-operative analgesic effect of pre-emptive use of Pregabalin & Ketorolac in patients undergoing single level decompressive lumbar laminectomy. Subjects and Methods : It is randomised, prospective, double blinded study in which 75 patients of ASA physical status grade I and II scheduled for single level elective decompressive lumbar laminectomy (L2-3, L3-4, or L4-5) were enrolled in the study. They were then randomly divided into three groups of 25 each, group C (control), P (pregabalin) and K (Ketorolac) by chit-in box method.Patients in group C, P and K received placebo drug, 150 mg pregabalin tablet and 10 mg ketorolac tablet respectively one hour before surgery with a sip of water. The patients were followed up to 24hr in post-operative period for pain relief and pain scoring was done by Numerical rating scale. Results: NRS was statistically insignificant at 1, 4, 12 & 24 hr. Rescue analgesic consumption at 1hr, 4hr, 12hr and 24hr was statistically insignificant.12%, 4% and 4% patients experienced drowsiness in group C, P and K respectively.32%,12% and 16 % patients experienced nausea and vomiting in group C, P and K respectively. Significantly higher mean systolic blood pressure is observed in group C at 1hr, 4hr and 12hr when compared to group P and group K. Significantly higher mean diastolic blood pressure is observed in group C at 1hr when compared to group P and group K. Conclusion: It was found that Pregabalin and Ketorolac do not decrease post-operative analgesic consumption when compared to control. There is no difference in adverse effect profile between Pregabalin and Ketorolac.
Keywords
Pre-emptive analgesia, Pregabalin, Ketorolac, single level decompressive lumbar laminectomy
Introduction
All surgical procedures are associated with certain level of postoperative pain. It has been reported that more than 80% of patients experience acute postoperative pain after undergoing surgical procedures.[1,2] In the opinion of American society of anesthesiologists (ASA) task force, acute pain management in the perioperative setting is referred to as measures taken before, during, and after a procedure to reduce or eliminate post-operative pain before discharge.[3] Unrelieved post-operative pain can cause increase in morbidity in terms of delayed wound healing, increased hospital stays, risk of development of chronic persistent post-surgical pain, deep vein thrombosis, pulmonary embolism, myocardial infarction, pneumonia, insomnia, and psychological demoralization.[4,5,6] The main goals of pre-emptive analgesia are to decrease pain after tissue injury, to prevent central sensitization and to reduce the incidence of chronic pain.[7]
Pregabalin has anticonvulsant, antihyperalgesic, and anxiolytic properties and has been introduced as part of multimodal analgesia. Ketorolac is a nonsteroidal anti-inflammatory drug (NSAID) with potent analgesic effects and a relatively low incidence of side effects. Ketorolac reversibly inhibits cyclooxygenase and decreases the hypersensitisation of tissue nociceptors that occurs with surgery.
Vertebral disc prolapse or rupture is one of the main causes of low back pain for which lumber laminectomy surgery was performed. In our institute, it was performed endoscopically. The primary outcome of our study was to compare post-operative analgesic effect of pre-emptive use of pregabalin & ketorolac and secondary outcome was to compare decrease in post-operative rescue analgesic consumption and to observe adverse effects of study drugs in patients undergoing single level decompressive lumbar laminectomy.
Subjects and Methods
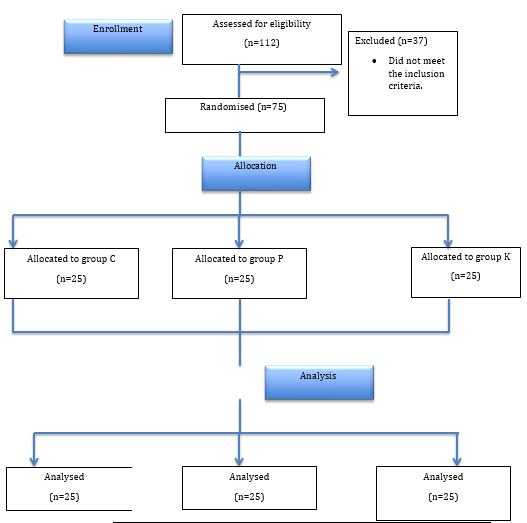
The institutional research and ethics committee approval was obtained. The current study included 75 ASA physical status I and II patients in age groups of 20-60 years, scheduled for single level elective decompressive lumbar laminectomy (L2-3, L3-4, or L4-5). They were then randomly divided into three groups of 25 each, group C (control), P (pregabalin) and K (Ketorolac) by chit-in box method [Figure 1].
A detailed history and systemic examination was carried out. Informed consent was obtained and patients were explained about numerical rating scale (NRS). The baseline vital parameters like pulse rate, systolic blood pressure, diastolic blood pressure, respiratory rate of all patients were recorded. Patients with known allergy or sensitivity to study group drugs, history of previous spinal surgery, hepatic insufficiency, renal insufficiency, pregnancy, preoperative analgesic management that include pregabalin & ketorolac in last 2 weeks prior to surgery, with uncontrolled hypertension (systolic blood pressure >180 mm of Hg or diastolic blood pressure >100 mm of Hg) and uncontrolled diabetes (random blood sugar >180 mg) were excluded from the study.
Patients in group C, P and K received placebo drug, 150 mg pregabalin tablet and 10 mg ketorolac tablet respectively one hour before surgery with a sip of water. The study drug or placebo was administered by an anaesthesiologist who was not involved in study.
Standard monitors included electrocardiogram, pulse oximetry, capnography & non-invasive blood pressure were attached in the operating room. Intravenous fluid, normal saline and ringer lactate were administered at the rate of 80 – 120ml/hr. Pre-medication was done with an intravenous injection of glycopyrolate 0.2 mg, midazolam 1 mg, ondansetrone 4 mg, hydrocortisone 100 mg and dexamethasone 8 mg. Analgesia was provided with an intravenous injection of fentanyl 2 microgram/kg. Induction of anesthesia was done with an intravenous injection of 2.5% thiopentone sodium 3-5 mg/kg and atracurium bromide 0.5 mg/kg. Mask ventilation was carried out till adequate relaxation achieved. Orotracheal intubation was done with appropriate size endotracheal tube. All patients were positioned prone following induction of anesthesia and pressure points were adequately padded. Local infiltration of surgical site with 15ml, 1% lignocaine with adrenaline (1 in 200000) was done 10 min prior to incision. Anaesthesia was maintained with sevoflurane (0.8 - 1 % end tidal concentration), Nitrous oxide and oxygen mixture (60:40), intravenous infusion of propofol at 50 – 70 microgram/kg/min and atracurium bromide infusion at 5 microgram/kg/min. At the end of surgery, patients were extubated after the reversal of neuromuscular blockade with an intravenous injection of neostigmine 0.05 mg/kg and glycopyrolate 0.01 mg/kg.
The patients were followed upto 24hr in the post-operative period for pain relief by anaesthesiologist blinded to patient groups and pain scoring was done by NRS at 1hr, 4hr, 12hr and 24hr.
Post-operatively all patients received paracetamol 15 mg/kg intravenously at 6 hr intervals. Diclofenac sodium 75mg in 100ml, 0.9% normal saline was used as rescue analgesic whenever the patient complained of pain (NRS >3 with associated hemodynamic changes). Patients with history of allergy to diclofenac sodium received an injection of tramadol 100mg in 100ml, 0.9% normal saline. All patients received an injection of ondansetrone 4 mg at 12 hr interval.
Statistical Analysis
Sample size was calculated at power 80% and alpha error 0.05 assuming standard deviation of 1.3 in pain score after extubation. It was further enhanced and rounded off to 25 cases equally divided into each group.
A statistical analysis was conducted using computer software (SPSS version 20 and primer). The qualitative data were expressed in proportion and percentages and the quantitative data were expressed as mean and standard deviations. The difference in mean was analysed by using student-t-test. One-way ANOVA, Post hoc test, TUKEY test was used for further analysis of data. Significance levels for tests were determined as 95% (P< 0.05).
Results
All seventy-five patients included in study were analysed. Groups were comparable with respect to their age, gender, height, weight, duration of surgery, ASA classification and level of Laminectomy [Table 1].
All patients were comparable regarding their pre-operative hemodynamic variables among the groups. No significant difference was observed in pre-operative heart rate, blood pressure and respiratory rate among all three groups (p Value > 0.05)
Intra-operative heart rate, SBP and DBP was recorded at every 30 min interval till surgery completed. No significant difference was observed among all three groups at 0 min, 30 min, 60 min, 90 min, 120 min, 150 min and 180 min (p value >0.05).
Post-operatively the heart rate, SBP and DBP was recorded at 1 hr, 4hr, 12 hr and 24 hr. Mean heart rate in Group C, Group p and Group K instead of Group A, Group B and Group C.
Mean SBP was 139.12, 131.12 and 132 mm of Hg at 1 hr, 131.28, 124.8 and 126.24 mm of Hg at 4 hr, 124.64, 120.72 and 121.28 mm of Hg at 12 hr and 121.12, 117.92 and 118.56 mm of Hg at 24 hr in group C, P and K respectively. It was statistically significant at 1hr (p value = 0.019), 4 hr (p value = 0.016), 12 hr (p value = 0.019) and statistically insignificant (p value = 0.122) at 24 hr [Table 2].
Mean DBP was 85.76, 79.2 and 81.12 mm of Hg at 1 hr, 76.8, 76.72 and 75.4 mm of Hg at 4 hr, 75.2, 73.68 and 72.8 mm of Hg at 12 hr and 73.32,72 and 71.68 mm of Hg at 24 hr in group C, P and K respectively. It was statistically significant at 1hr (p value = 0.016) and statistically insignificant at 4, 12 and 24 hr [Table 3].
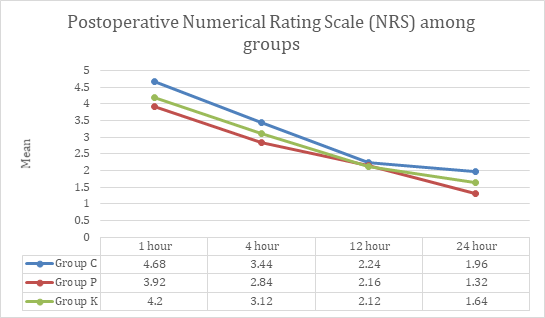
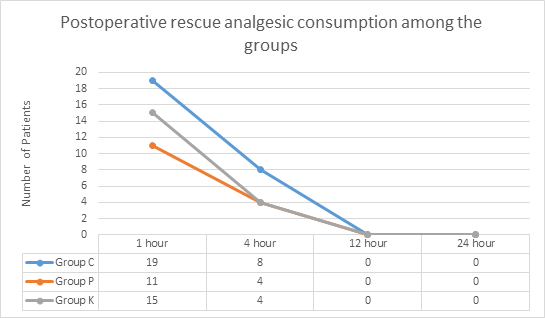
NRS was statistically insignificant at 1, 4, 12 & 24 hr.Rescue analgesic consumption at 1hr, 4hr, 12hr and 24hr was statistically insignificant. At 12hr and 24hr, none of the patients in group C, P and K needed rescue analgesia (p value >0.05) [Figure 2].
12%, 4% and 4% patients experienced drowsiness in group C, P and K respectively.32%,12% and 16 % patients experienced nausea and vomiting in group C, P and K respectively. None of study patients had complained of surgical site oozing. Although, the percentage of patients with adverse effects was higher in group C, it was statistically insignificant (p value >0.05) [Figure 3].
|
|
Group C (n = 25) |
Group P (n = 25) |
Group K (n = 25) |
p Value |
|
Age (in years) |
48.24 ± 11.72 |
40.96 ± 12.67 |
42.48 ± 12.12 |
0.09 |
|
Gender |
|
|
|
|
|
Male |
8 (32%) |
4 (16%) |
11 (44%) |
0.098 |
|
Female |
17 (68%) |
21 (84%) |
14 (56%) |
|
|
Height (in cm) |
165.44±5.796 |
164.98±5.454 |
162.84±6.78 |
0.319 |
|
Weight (in Kg) |
73.52 ± 7.001 |
72.84 ± 13.474 |
67.6 ± 8.746 |
0.084 |
|
Duration of Surgery (in min) |
145.20±17.263 |
146.36±16.928 |
142.84±16.476 |
0.755 |
|
ASA Classification |
|
|
|
|
|
I |
9 (36%) |
14 (56%) |
13 (52%) |
0.326 |
|
II |
16 (64%) |
11 (44%) |
12 (48%) |
|
|
Level of Laminectomy |
|
|
|
|
|
L 3-4 |
1 (4%) |
6 (24%) |
7 (28%) |
0.066 |
|
L 4-5 |
24 (96%) |
19 (76%) |
18 (72%) |
|
|
Systolic Blood Pressure (mmHg) |
1 hr |
4 Hr |
12 Hr |
24 Hr |
|
|
Group C |
Mean |
139.12 |
131.28 |
124.64 |
121.12 |
|
SD |
9.488 |
7.323 |
4.957 |
5.747 |
|
|
Group P |
Mean |
131.12 |
124.8 |
120.72 |
117.92 |
|
SD |
10.879 |
8.446 |
5.443 |
5.671 |
|
|
Group K |
Mean |
132 |
126.24 |
121.28 |
118.56 |
|
SD |
11.762 |
8.531 |
5.128 |
5.846 |
|
|
P Value |
0.019 |
0.016 |
0.019 |
0.122 |
|
|
Diastolic Blood Pressure (mmHg) |
1 hr |
4 Hr |
12 Hr |
24 Hr |
|
|
Group C |
Mean |
85.76 |
76.8 |
75.2 |
73.32 |
|
SD |
7.601 |
6.76 |
4.397 |
4.75 |
|
|
Group P |
Mean |
79.2 |
76.72 |
73.68 |
72 |
|
SD |
7.916 |
7.12 |
5.375 |
4.546 |
|
|
Group K |
Mean |
81.12 |
75.4 |
72.8 |
71.68 |
|
SD |
8.584 |
5.71 |
3.512 |
4.069 |
|
|
P Value |
0.016 |
0.68 |
0.168 |
0.392 |
|
Discussion
The current study was aimed to assess and compare post-operative analgesic effect of pre-emptive use of pregabalin & ketorolac in patients undergoing single level decompressive lumbar laminectomy. Opioid analgesics continue to play an important role in the acute treatment of moderate to severe pain in the early post-operative period. The problems with these drugs are variety of post-operative side effects which tend to inhibit rapid recovery and rehabilitation. Hence, the search for new analgesic agents like pregabalin, ketorolac and others continues, which reduces requirement of opioids. Ideal analgesic agent has same analgesic potency as that of opioids but without their side effects.
From the results of the current study, it can be said that ketorolac and gabapentin, decrease opioids requirement and may decrease the incidence of side effects when compared to opioids but it is statistically insignifcant compared to the control group.
These results are in contrast to the study done by D Pavelescu et al.[8] who studied the efficacy of 2 drugs ‐ Pregabalin and Ketorolac ‐ in a multimodal analgesic regimen, against a placebo‐control group in patients undergoing surgery for carpal tunnel syndrome. They found that multimodal analgesic regimen not only help in improving analgesia and patient comfort but also prevent the development of chronic pain after carpal tunnel syndrome surgery by stopping central hemoplastic changes. Also, in another study Nella A. et al.[9] found that single pre-operative dose of Pregabalin seems to enhance the recovery after surgery for Inflammatory Bowel Disorder in term of pain & anxiety.
Nuno Nistal B. et al.[10] studied pre-emptive analgesic effect of Ketorolac for abdominal hysterectomy. They concluded that pre-operative Ketorolac did not show a pre-emptive analgesic effect. It was not effective as an adjuvant to decrease opioid requirement or post-operative pain in patients receiving intravenous analgesia with Tramadol after abdominal hysterectomy.
In our study there was no significant difference in post-operative changes in heart rate per minute among the groups at 1hr, 4hr, 12hr and 24hr.
Systolic blood pressure and diastolic blood pressure were also recorded at 1hr, 4hr, 12hr and 24hr. significantly higher mean systolic blood pressure was observed in group C at 1hr, 4hr and 12hr as compared to group P and group K. The rise in systolic blood pressure might be due to pain in group C patients at 1hr, 4hr and 12hr. There was no significant difference in mean systolic blood pressure at 24hr. There was significantly higher mean diastolic blood pressure in group C at 1hr as compared to group P and group K. This difference might be due to pain in group C patients at 1hr. There was no significant difference in mean diastolic blood pressure at 4hr, 12hr and 24hr.
Nuno Nistal B et al.[10] indicated that there were no differences in hemodynamic parameters including blood pressure post-operatively in study group those who received Ketorolac.
There was a gradual decrease in the NRS recording among all the groups. However, these were not statistically significant.
Zengin U et al.[11] Macheridou A et al,[12] Nella A et al,[9] Balaban F et al,[13] favoured the effectiveness of pre-emptive Pregabalin and Ketorolac for decreasing pain score.
Rescue analgesic consumption was recorded at 1hr, 4hr, 12hr and 24hr. At 1hr, 11 patients in group P, 15 patients in group K and 19 patients in group C needed rescue analgesic. At 4hr, 4 patients in group P, 4 patients in group K and 8 patients in group C needed rescue analgesic. At 12hr and 24hr, none of the patients in group P, K and C needed rescue analgesic. There was no significant difference in post-operative rescue analgesic consumption among the study groups.
Similar study was done by Nuno Nistal B et al,[10] & C Vanlersberghe et al,[14] which indicated that pre-emptive Ketorolac had no effect on rescue analgesic consumption.
Another study by Zengin U et al,[11] Macheridou A et al,[12] and others demonstrated the positive effect of pre-emptive Pregabalin on rescue analgesic consumption.
The limitations of the current study are the small sample size which is not adequate to draw valid conclusions concerning the safety profile of the analgesic interventions.
Conclusion
Pregabalin and Ketorolac do not decrease post-operative analgesic consumption as compare to control (p value > 0.05). There is no difference in between Pregabalin and Ketorolac to decreases post-operative analgesic consumption (p value > 0.05).
Also, no difference in adverse effect profile between Pregabalin and Ketorolac (p value>0.05).